Stefan Rose, M.D.: The Forensic Unreliability of Retrograde Extrapolation in Antemortem Cases
Pharmacokinetics is the branch of pharmacology that deals with the concentration of ethanol (or any drug) in the blood (or any other tissue) at any given point in time. When the blood alcohol concentration (BAC) is of importance in a legal case one can distinguish two types of BAC cases, antemortem (before death) and postmortem (after death) cases.
In antemortem cases, usually a blood sample is obtained from a person some time after an incident has occurred, often an hour or more. The BAC result is for that sample drawn at that time. It does not predict the BAC at any other time, especially at the time of the incident.
Many times an estimation of the BAC at the time of the incident will be attempted. This estimation is called “retrograde extrapolation”. Retrograde extrapolation is not a standard term used in medical pharmacology but is widely used in forensic cases. Its most serious limitation is that two facts must be known to perform this retrograde extrapolation. One must know if the person has completely absorbed all the ethanol beverage that was consumed during the drinking episode (from their gut into their bloodstream), and one must know the persons ethanol elimination rate per hour.
That information is usually incomplete or unknown. Therefore any attempt at estimating a BAC backwards in time from a BAC test result has been called “dubious” and “speculative” by other investigators in the field. 1,2
Before any pharmacokinetic opinion can be made, the BAC test results must be inspected for accuracy and reliability. If the BAC test results are inaccurate or otherwise unreliable then no meaningful retrograde extrapolation may be performed.
Let’s review this inspection process step by step.
Antemortem Cases
The first step in the workup of a forensic BAC case is to determine the type of blood sample tested. The types of blood samples include venous whole blood, arterial whole blood, serum and plasma. Venous whole blood is the standard blood sample that should be used in forensic blood ethanol cases. The reasons for using venous whole blood include:
- Whole blood is often a government regulated requirement in criminal cases.
- Serum or plasma, which is whole blood minus the red blood cells, white blood cells and platelets, contains more water per unit volume (i.e., milliliter) than the original whole blood sample. The extra water contains more ethanol per milliliter compared to the whole blood it was derived from. The amount of extra ethanol is variable, from about 10% to 50%, so there is not a single conversion factor to transform a serum or plasma ethanol result to its comparable whole blood concentration.3
- Arterial blood is sometimes drawn in blood alcohol cases, but this type blood sample is not reliable for ethanol determination. Arterial blood is the blood that has absorbed ethanol from the gut and is delivering the ethanol to the peripheral tissues (muscles, organs and the brain). During the absorption of ethanol from the gut, the arterial blood has a higher concentration of ethanol than venous blood, variable and up to 40% higher. 4 Therefore the arterial blood is an unreliable sample for ethanol determination.
If the sample is unreliable, then any attempt to estimate a venous whole blood BAC at any point in time will also be unreliable, and the retrograde analysis should stop at this juncture.
The second step in the forensic BAC case workup is a review of the laboratory litigation package of documents. A complete litigation package will help the reviewer decide both the accuracy and the reliability of the BAC analysis. The litigation package should contain enough information for the reviewer to determine at least the following:
- The sample tested (whole blood, serum, plasma, other)
- The method of analysis (GC-FID, GC-FID-MS)
- Method validation
- Quality control performance for that batch
- Uncertainty calculation with back up documentation
If the litigation documents do not support an accurate or reliable test result, then any retrograde extrapolation will not be accurate or reliable and the retrograde analysis should stop at this point.
The third step in the forensic BAC case workup is to ascertain whether or not the person was still absorbing ethanol at the time of the driving. Absorption is when alcohol beverage is present in the stomach and small intestine (the “gut”). A process called diffusion occurs to transfer the alcohol beverage from the gut into the bloodstream. This diffusion occurs mostly in the small intestine, so the majority of alcohol beverage is absorbed into the bloodstream from the small intestine. Very little is absorbed from the stomach.
Absorption of alcohol beverage into the bloodstream can be measured by the total amount of time it takes to empty the gut of the alcohol beverage. That is called the absorption interval and may last for many hours depending on several variables. The absorption interval is variable from person to person and with the same person, depending on the variables present. Those variables include the individual’s genetic profile, prior illness, current illness, current medications, nicotine use, and of course the presence of food in the gut. The major controller for the absorption interval affected by those variables is the pyloric valve, located at the end of the stomach. It opens and closes and allows stomach contents to enter the small intestine, for absorption into the bloodstream.
Absorption can also be measured by how fast the blood alcohol level increases per unit time (per minute, per hour) and is called the absorption rate. This measurement is dependent on the opening of the pyloric valve but also by how fast the stomach contents are transferred into the bloodstream by diffusion in the small intestine. Diffusion is governed by “Fick’s Law of Diffusion” and is variable from person to person. 5,6
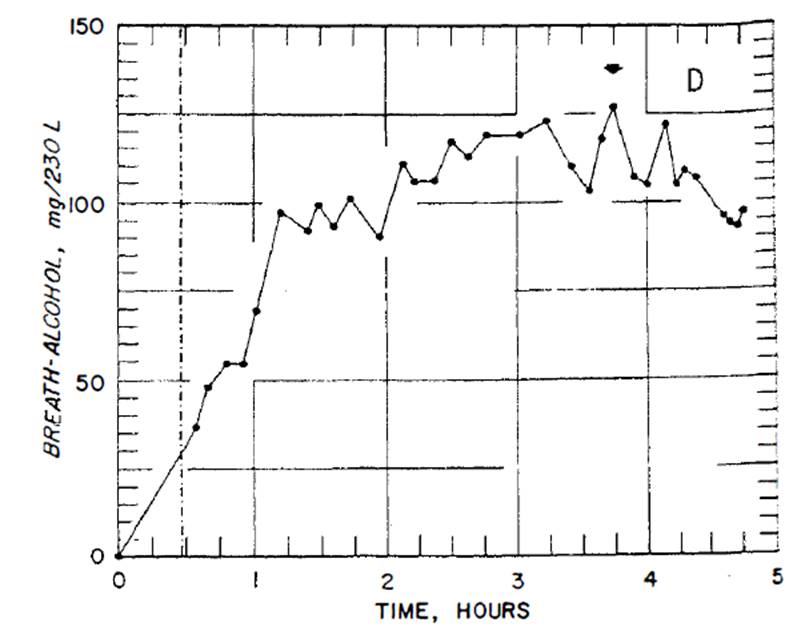
In conclusion the absorption interval may last for hours and the absorption rate may be fast or slow in any given person during any given drinking episode. The interval and rate are quite variable, not predictable, and the only way to determine a person’s absorption status is by taking sequential timed blood samples from the time of the incident, measuring the BAC and looking at the results to see if they are increasing (still absorbing), at a plateau (still absorbing) or declining (in the elimination phase). Without that information it is not possible to predict if a person is still absorbing ethanol at the time of the incident and or after the incident.
If the absorption status of a person is not known then any attempt to estimate a venous whole blood BAC at any point in time will be unreliable, and the retrograde analysis should not be performed.
Representative BAC graphs demonstrating the extreme variability of BAC absorption are shown below. 7

References
- Jones, A.W., 1988, “Problems and pitfalls with backtracking BAC to the time of driving”, DWI Journal : law & science, 3:6, 8-12
- Dubowski, K.M., 1976, “Human Pharmacokinetics of Ethanol”, Alcohol Technical Reports, Vol. 5, No. 4, 55-63
- Rainey, P.M., 1993, “Relation between Serum and Whole-Blood Ethanol Concentrations”, Clinical Chemistry, Vol. 39, No. 11, 2288-2292
- Garriott’s Medical Legal Aspects of Alcohol, Fifth Edition, Chapter six, pg. 218
- http://web.mit.edu/1.061/www/dream/ONE/ONETHEORY/onetheory.htm
- “Chapter 1. Functional Anatomy of the GI Tract and Organs Draining into It.” Gastrointestinal Physiology, 2e Ed. Kim E. Barrett. McGraw-Hill, 2014
- Dubowski, K.M., 1985, “Absorption, Distribution and Elimination of Alcohol: Highway Safety Aspects”, Journal of Studies on Alcohol, Supplement No. 10, July 1985